UK Engineer Designs Own Life-Saving Implant, 20 Patients Follow
Share
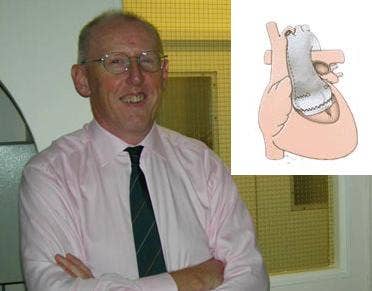
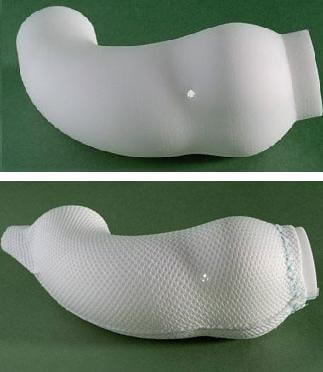
In the six years since Tal Golesworthy had the implant he designed inserted into his own chest, his device has saved the lives of more than twenty others. The ExoVasc Aortic Root Support isn't much to look at, just a cloth-like mesh about the size of your thumb, but Golesworthy designed it in a way that was revolutionary for the time. He used MRI scans, CAD, and rapid prototyping to build a complete model of his ill and dilating aorta artery on his heart. With that model he helped doctors create the ExoVasc, a containment that would keep his aorta from expanding, and keep him alive. Now, through his company Exstent LTD, and the work of some of the same surgeons who implanted him, Golesworthy is sharing his engineering insights with others who suffer from his condition. His is a tale that shows how, with accelerating technology, individuals increasingly have the power to shape their own medical destiny.
Golesworthy suffers from Marfan Syndrome, a genetic disorder that affects connective tissue in the body, often leading to an aorta that dilates until it is dangerously large, sometimes to the point of rupturing. Marfan is estimated to affect between 1 in every 3000 to 5000 people. Patients like Golesworthy who have dilating aortas often face two options: risk a major heart attack or undergo the Bentall Procedure, a five hour surgery with heart-lung bypass, that replaces the aorta with a graft and mechanical valve. After Bentall surgery, patients must spend the rest of their lives on anti-coagulants.
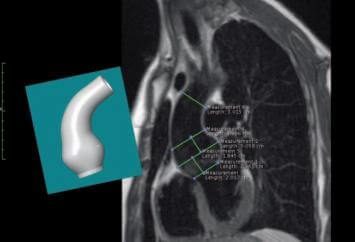
When Golesworthy faced that decision in 2000 he chose option C: frak it all and make up a new procedure. Over the next four years he would work with Tom Treasure at Guy's Hospital and John Pepper at the Royal Brompton Hospital to find an alternative solution. Golesworthy hit upon the idea of using MRI imaging, and CAD to build a digital model of his aorta. They could then print that model using rapid prototyping. With his custom-built faux aorta in hand, Golesworthy,Treasure, Pepper and others could then design a containment system that would exactly fit his dilated artery. They created a textile mesh that weighed less than five grams and that surgeons could be certain would fit him on the first try. (A previous attempt to use a mesh on another patient had failed because the containment had to be fitted during the surgery.) In 2004 Golesworthy went under the knife and had the first ExoVasc implanted.
If that was the end of the story I'd still be impressed, but Golesworthy continued with his new colleagues to replicate his journey for others. There were many patients with Marfan Syndrome (some 12,000 or so in the UK) and many would face the Bentall Procedure dilemma. Since 2004, 23 patients were given the ExoVasc. Golesworthy didn't just save his own life, he saved others as well. And more are on the way. The device ended clinical trials in 2009, seven more patients are lined up, and John Pepper at Royal Brompton Hospital is scheduled to continue performing/overseeing the surgeries.
Be Part of the Future
Sign up to receive top stories about groundbreaking technologies and visionary thinkers from SingularityHub.

Now, to be clear, this particular device isn't going to revolutionize heart surgery all on its own. The ExoVasc is only approved for a very particular kind of patient (one with Marfan and dilated aorta) and while very successful, it isn't perfect. As described in the Journal of the Royal Society of Medicine, while all of the first 20 patients survived the new operation, only 19 saw the planned benefits. Still, those are good odds, especially when you consider the advantages Golesworthy's device has over the Bentall Procedure. No heart/lung bypass. Two hours of surgery instead of five or more. No need to be on anti-coagulants for the rest of your life. We have a definite winner here, folks, even if the opportunities to use it are relatively small compared to the field of heart surgery as a whole.
The underlying principle to Golesworthy's actions, however, could be repeated often in the future. Advancing technologies are increasingly giving us the ability to understand and even treat our own medical conditions. Golesworthy has said that the medical field needs to better interface with engineers, and that it will be engineers who can help realize some of the technological dreams currently sitting on the cutting-edge of medicine. That's certainly true. Yet at some point accelerating technologies will allow many of us to assist in our own treatments even if we are not engineers. Search engines already help patients find journal articles that doctors may not have time to research on their own. Artificial intelligence enabled software will only improve that trend. Social networks of patients with the same condition may find trends that scientists haven't had time to explore. Rapid-prototyping is making its way in the home, and some hobbyists may already have access to 3D printers that their doctors do not. There will undoubtedly be countless other innovations that the discerning patient could leverage to help themselves and their medical professional create new solutions to their ailments.
This isn't something we should jump towards too brazenly. Golesworthy was in a dire condition and had his own expertise. Certainly it's too soon for most of us to design our own implants. Yet I think his situation shows how all of us could eventually play a larger part in designing our own healthcare. As technology continues to advance, more of us reach that point everyday.
[image credits: Exstent LTD]
[sources: Exstent, The Engineer, Pepper et al 2010 JRSocMed]
Related Articles

The Mad Scramble to Power AI Is Rewiring the US Grid

Chatbots ‘Optimized to Please’ Make Us Less Likely to Admit When We’re Wrong

Forget Antibiotics: These Killer Cells Wipe Out Deadly Superbugs in a Day
The Mad Scramble to Power AI Is Rewiring the US Grid
Chatbots ‘Optimized to Please’ Make Us Less Likely to Admit When We’re Wrong
Forget Antibiotics: These Killer Cells Wipe Out Deadly Superbugs in a Day
What we’re reading