AIDS Turns 30: Are We Close to a Cure?

Share
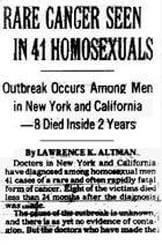
An early headline of the AIDS epidemic (New York Times, 1981). The condition made patients vulnerable to Kaposi's sarcoma, a rare cancer.
On June 5th, 1981, the Morbidity and Mortality Weekly Report told the world about five rapidly deteriorating men who arrived at clinics in Los Angeles. They exhibited a disturbing array of symptoms - swollen lymph nodes, skin rashes, and failing immune systems. At the time of publication, two patients had already died. The scourge that we now know as AIDS had begun.
Three decades, volumes of research papers, and 30 million deaths later, we’ve learned much about this killer retrovirus, yet an actual cure remains an unrealized dream for the millions currently infected worldwide. In the ongoing conflict of host vs. pathogen, no adversary has proved more tenacious than HIV. Why?
For one, HIV has a high evolutionary potential - rapidly altering its gene sequences to build drug resistance and avoid detection from vaccines. In fact, there are at least 93 common mutations that make HIV drug-resistant. Once you nail down one subtype of HIV, another one invariably pops up. Also, HIV is a retrovirus than can integrate with the host's genome. The virus is so inextricable because it literally becomes a part of the afflicted. Furthermore, it's a master of hide-and-seek, evading the effects of drugs by hiding in lymph nodes during clinical latency. Lastly, the virus disarms the immune system so other opportunistic infections can overrun the defenseless body. Amid this diabolical synergy of viral advantages, this malicious microbe has been one-upping the world's best scientists for thirty long years. And it's a battle we're currently losing. According to the latest UN reports, for every two patients who start taking anti-HIV drugs, there are five new infections.
The red ribbon has come to represent the solidarity of individuals and families living with HIV. Hopefully, in my lifetime, this powerful symbol will become a relic of the past when HIV is snuffed out of existence. Here's to hoping.
Nonetheless, HIV's days on the winning side could be numbered. Multiple paths toward a cure and eradication are sprouting, and the headlines seem to imply that we're closing in on a solution. So, what are those paths, and how will they help us get there?
When it comes to vanquishing a disease, there are two ways to skin a cat – treating the illness post-infection or preventing transmission. In the case of HIV, early and aggressive treatment can also be a highly effective prophylactic measure. According to early results from a landmark study led by Myron Cohen at UNC-Chapel Hill, rapid deployment of antiretrovirals (ARVs) – drugs that suppress HIV infection and slow the progression to AIDS – caused a 96% reduction in transmission. It just goes to show that early detection and treatment are key, and sometimes the best defense is a good offense.
Dr. Myron Cohen of UNC shows we can significantly curb HIV using the tools we already have.
As promising as this approach seems, there are some limitations to consider. To see a real impact of early ART on a global scale and consistently catch HIV in the early stages, testing needs to be cheap, fast, ubiquitous, de-stigmatized, and occur on a regular basis. Sobering impracticality currently makes this exceedingly difficult, and even post-industrial nations have issues getting their people tested. There's also the financial burden of HIV treatment. While a cost drop followed the introduction of generic drugs, there’s still a dire need for more cost-effective ARV regimens. If people don’t have access to the drugs, early ART is dead in the water.
It won’t be able to eradicate HIV on its own, but perhaps fine-tuning ART regimens will help give HIV a major wallop, provided that costs of testing and drugs are sufficiently mitigated. With greater access to ARVs and the falling cost of bioassays, there’s plenty reason to be hopeful on this front.
Optimized ART and promising new vaccines bring us closer toward AIDS abolition on the population level, but they mean nil to the ones who’ve been HIV positive for years. For these individuals, the outlook is much better than it was in the 1980s, but the quality of life can still be grim. Enter the “Berlin patient,” a man functionally cured of HIV with stem cells from the bone marrow of an immune donor. It was an amazing proof-of-concept, but the operation was not without difficulties. Aside from genetic compatibility snags, harvesting can be painful, discouraging donating and constricting the marrow pool.
Be Part of the Future
Sign up to receive top stories about groundbreaking technologies and visionary thinkers from SingularityHub.

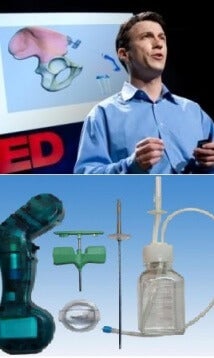
Daniel Kraft presenting the Marrow Miner at TED in 2009.
Fortunately, on the side of marrow harvesting, the future is already looking brighter. A few years ago, Daniel Kraft, a Stanford physician-scientist and Singularity University track chair, invented the cleverly-coined Marrow Miner. Not only can it gather up to six times more adult stem cells than traditional methods, it’s far less invasive and can be performed in an outpatient setting. It probably won’t make bone marrow donation as popular as blood drives, but it could make it a hell of a lot easier and donor-friendly than it used to be. With more stem cells to choose from and a greater chance of genetic compatibility, there could be more “Berlin patients” waiting in the wings.
But why even risk compatibility snags when you can use your own genetically enhanced stem cells? Way back in 2009, Singularity Hub reported on one gene therapy trial that boosted CD4+ counts by infusing HIV patients’ blood cells with virus-impeding genes. The results were nothing to sneeze at, but the technique only replaced a fraction of the cells, leaving the remainder vulnerable to a viral rebound. The trick is giving the immune system a complete genetic remodeling - a challenge elegantly reviewed in a recent issue of Human Molecular Genetics.
It’s very easy to be enthralled by stem cell and gene therapies for HIV, but as we've seen, there are still many barriers to overcome. To put things into perspective, the FDA has yet to approve a single gene therapy for any disease, HIV or otherwise. Gene therapy and stem cell research appear to be creeping forward phlegmatically, but the mountaintop is within the sights of scientists. They might just need a pair of binoculars at this point.
The 30 year struggle against AIDS has been a grueling one. Glimmers of hope from the research community have faded into unfulfilled promises, turning the barrage of “breakthrough!” headlines into some sort of a cruel joke. However, as futurephiles, we at the Hub recognize the paramount role that long-term trends play in the shaping of humanity’s destiny. And so far, the trend has been a good one. HIV was once an imminent death sentence, but can now be held at bay for decades. On the horizon, platform biotechnologies are paving the way to new treatments. Even so, we should not underestimate the existential risk posed by emergent viruses, both man-made and naturally occurring. Futurist Nick Bostrom posed the question in his seminal paper: "What if AIDS was as contagious as the common cold?" While this may deviate from the pathogen's optimal virulence, it is a prospect that sends chills down my spine. If we don’t keep these bugs in check, then these lofty notions of cybernetics, life-extension, and Singularity could become a fool’s dream, and the great achievements of humanity would blow away like dust in the wind. We can’t let that happen. We’ve come too far to let HIV or any other virus stand in our way. Microbes, you’ve been warned.
While the seer speaks of greener pastures on the other side, the microbial menace lurks 'neath the bridge, threatening those who dare to cross.
[Images Credits: 1. The New York Times 2. Healthplanone.com (modified)3. UNC 4. TED 5. Wikimedia Commons, Microsoft Clip Art (modified) ]
[Sources: Morbidity and Mortality Weekly Report, AVERT, The Lancet, New Scientist, Human Molecular Genetics, Science Insider]
Related Articles

Japan Thinks Swarms of Transformer Robots Could Explore the Moon
")
This Week’s Awesome Tech Stories From Around the Web (Through June 13)

Is Richard Dawkins Right About Claude? No. But It’s Not Surprising AI Chatbots Feel Conscious to Us.
Japan Thinks Swarms of Transformer Robots Could Explore the Moon
This Week’s Awesome Tech Stories From Around the Web (Through June 13)
Is Richard Dawkins Right About Claude? No. But It’s Not Surprising AI Chatbots Feel Conscious to Us.
What we’re reading