Who Should Get a Covid-19 Vaccine First?

Share
If the book of nature is written in the language of mathematics, as Galileo once declared, the Covid-19 pandemic has brought that truth home for the world's mathematicians, who have been galvanized by the rapid spread of the coronavirus.
So far this year, they have been involved in everything from revealing how contagious the novel coronavirus is, how far we should stand from each other, how long an infected person might shed the virus, how a single strain spread from Europe to New York and then burst across America, and how to "flatten the curve" to save hundreds of thousands of lives. Modeling also helped persuade the Centers for Disease Control and Prevention that the virus can be airborne and transmitted by aerosols that stay aloft for hours.
And at the moment many are grappling with a particularly urgent—and thorny—area of research: modeling the optimal rollout of a vaccine. Because vaccine supply will be limited at first, the decisions about who gets those first doses could save tens of thousands of lives. This is critical now that promising early results are coming in about two vaccine candidates—one from Pfizer and BioNTech and one from Moderna—that may be highly effective and for which the companies may apply for emergency authorization from the Food and Drug Administration.
But figuring out how to allocate vaccines—there are close to 50 in clinical trials on humans —to the right groups at the right time is “a very complex problem,” says Eva Lee, director of the Center for Operations Research in Medicine and Health Care at the Georgia Institute of Technology. Lee has modeled dispensing strategies for vaccines and medical supplies for Zika, Ebola, and influenza, and is now working on Covid-19. The coronavirus is “so infectious and so much more deadly than influenza,” she says. “We have never been challenged like that by a virus.”
Howard Forman, a public health professor at Yale University, says "the last time we did mass vaccination with completely new vaccines," was with smallpox and polio. "We are treading into an area we are not used to." All the other vaccines of the last decades have either been tested for years or were introduced very slowly, he says.
Because Covid-19 is especially lethal for those over 65 and those with other health problems such as obesity, diabetes, or asthma, and yet is spread rapidly and widely by healthy young adults who are more likely to recover, mathematicians are faced with two conflicting priorities when modeling for vaccines: Should they prevent deaths or slow transmission?
The consensus among most modelers is that if the main goal is to slash mortality rates, officials must prioritize vaccinating those who are older, and if they want to slow transmission, they must target younger adults.
"Almost no matter what, you get the same answer," says Harvard epidemiologist Marc Lipsitch. Vaccinate the elderly first to prevent deaths, he says, and then move on to other, healthier groups or the general population. One recent study modeled how Covid-19 is likely to spread in six countries—the US, India, Spain, Zimbabwe, Brazil, and Belgium—and concluded that if the primary goal is to reduce mortality rates, adults over 60 should be prioritized for direct vaccination. The study, by Daniel Larremore and Kate Bubar of the University of Colorado Boulder, Lipsitch, and their colleagues, has been published as a preprint, meaning it has not yet been peer reviewed. Of course, when considering Covid-19's outsized impact on minorities—especially Black and Latino communities—additional considerations for prioritization come into play.
Most modelers agree that "everything is changing with coronavirus at the speed of light," as applied mathematician Laura Matrajt, a research associate at the Fred Hutchinson Cancer Research Center in Seattle, put it in an email. That includes our understanding of how the virus spreads, how it attacks the body, how having another disease at the same time might raise the risk, and what leads to super-spreader events.
"Because vaccine supply will be limited at first, the decisions about who gets those first doses could save tens of thousands of lives."
So far, the research has yielded some surprising results. While children are usually prioritized for flu vaccine, for example, experts say the very young should be a lower priority for Covid-19 vaccines in the United States, because thus far young adults have been primary drivers of transmission. (This is not necessarily true across the globe; in India, for instance, where multiple generations often live together in smaller spaces, new research shows both children and young adults are spreading much of the virus in the two states studied).
In addition, several models suggest that significant headway can be made against the pandemic even with lower deployment of a vaccine that is only partly effective. And several others emphasize the importance of local infection and transmission rates. According to Lee, whose early assessments of the pandemic's origin, virulence, and probable global trajectory proved to be strikingly accurate, New York could potentially contain the virus if about 40 percent of the population were vaccinated, because local transmission of the virus is fairly low (a positivity rate of a little below 3 percent as of Nov. 16), and around 20 percent have already been infected.
"The higher the fraction of people in the population who already have antibodies, the more bang for your buck," says Larremore, because you can prioritize giving vaccines to those who don’t have antibodies.
All these findings are important because, "at the end of the day, you will never have enough vaccines for the entire population," says Lee—and not all Americans will take it. In fact, the World Health Organization recently predicted that healthy young adults may not even be able to get a vaccine until 2022, after the elderly, health care workers, and other high-risk groups are vaccinated.
....
To model the rollout of vaccines, mathematicians must build formulas that reflect the starburst of human life and our complex interactions, using data like housing and socioeconomic status, daily habits, age, and health risks. But first they establish how contagious the virus is—its reproductive rate, or "R-naught." This represents the number of people that one infected person can be expected to transmit the infection to.
When some fraction (depending on R-naught) of people are immune (either by recovering from natural infection, if that grants immunity, or through vaccination), herd immunity has been achieved. That means that while small outbreaks may still occur, the pandemic will not take off globally again. Given the R-naught of SARS-CoV-2, the virus that causes Covid-19, the World Health Organization has estimated that 65 percent to 70 percent of the population needs to be immune before this can be achieved.
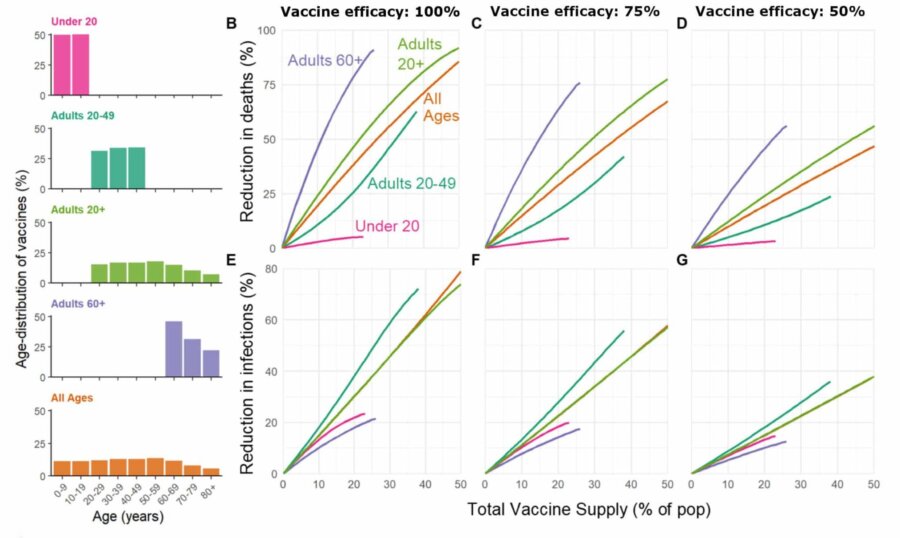
Vaccine rollout scenarios developed by Bubar et al. include five different ways of distributing the first doses of vaccines, presented in the left panel. The scenarios show the same pattern: to prevent deaths, vaccinate the elderly first, and then move on to other, healthier groups or the general population. Visual: Bubar et al. / MedRxiv
Modeling vaccine rollout requires a complex acrobatics, and while the models to flatten the curve that mesmerized the public last spring took weeks to craft, vaccine distribution models take many months. There are innumerable practical challenges facing modelers.
For one thing, many of the vaccines currently in the pipeline—including the two candidates from Pfizer and BioNTech and Moderna—require two shots, several weeks apart, which involve registries and follow-up to ensure that people get the second, critical booster shot. And as the New York Times noted in late September, "Companies may have to transport tiny glass vials thousands of miles while keeping them as cold as the South Pole in the depths of winter."
There is also the question of vaccine efficacy. Will a given vaccine provide robust immunity, and in all groups? Or will it primarily shorten duration of infection and lessen symptoms, which would still be of great value in reducing mortality as well as transmission? And what if a vaccine is less effective among the elderly, as is often the case? At the moment, vaccines using messenger RNA (including those produced by Moderna and Pfizer and BioNTech) are "looking pretty good in older adults," according to Kathleen Neuzil, director of the Center for Vaccine Development and Global Health at the University of Maryland School of Medicine. Preliminary analyses of both vaccine candidates show that they may be more than 90 percent effective.
Finally, there is also the vexing question of how long immunity might last after infection. For some viruses, such as the varicella-zoster virus that causes chickenpox, immunity can last for decades. For others, such as the family of coronaviruses that includes SARS-CoV-2 and the common cold, the virus has a relatively high mutation rate that may protect novel strains from our antibodies. That uncertainty is difficult to model precisely, so many modelers assume that, for the time being at least, those who have been infected are immune.
....
Matrajt, of the Fred Hutchinson Cancer Center in Seattle, remembers vividly how hard it was to begin to construct a model out of thin air when she began working with colleagues on a vaccination model this past April. There were "so many uncertainties," she recalls. Together, the researchers developed algorithms based on an astonishing 440 or so combinations of parameters, from transmission to immunity to age groups and mortality. Their computers spent nearly 9,000 hours running equations, and their model, published in August as a preprint, shows that if there is only a low supply of vaccine at first, older adults should be prioritized if the goal is to reduce deaths.
But for vaccines that are at least 60 percent effective, once there is enough to cover at least half the population, switching to target healthy individuals ages 20 to 50 as well as children would minimize deaths. The model also predicts how many deaths can be averted with different amounts of vaccine coverage. For instance, if 20 percent of the population has already been infected and is immune, deaths could be halved by vaccinating just 35 percent of the remainder, if the vaccine is at least 50 percent effective.
In the model by Matrajt and her colleagues, herd immunity is achieved once 60 percent of the population is immune. "It is completely normal that different models will give different numbers," she says, explaining why her estimate varies slightly from the WHO figure of 65 percent.
The model does "a really nice job looking at a large number of plausible cases," says Michael Springborn, an environmental and resource economist at the University of California, Davis, who just finished his own model with Jack Buckner, a colleague at UC Davis, and Gerardo Chowell, a mathematical epidemiologist at Georgia State University. Their study, released in preprint, also suggests the power of careful initial targeting in reducing deaths.
The models suggest that even a partially-effective vaccine given to just part of the population, says Springborn, "can go a really long way to reducing infections and reducing deaths."
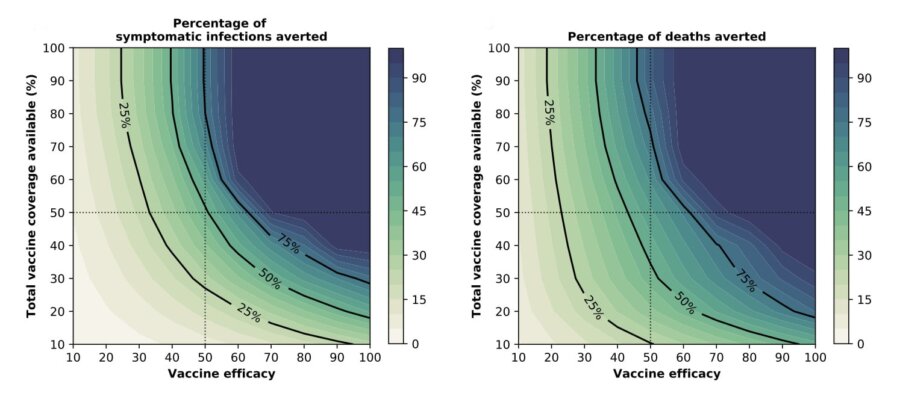
A vaccine rollout model by Matrajt and her colleagues shows how availability and efficacy of the vaccine affects infections and deaths due to Covid-19. Visual: Matrajt et al. / medRxiv
Lee's modeling, created with software she first developed in 2003, in conjunction with the CDC, for dispensing of supplies in natural disasters and pandemics, analyzes how the disease might be contained in areas with different infection rates and initially scarce vaccine supplies. In New York City, which was hit so hard in the spring, her model predicts that roughly 60 percent of the population may need immunity to contain the pandemic. Assuming 20 percent are already infected, about 40 percent would need to be vaccinated. In San Diego, however, where infection rates have been lower, Lee’s model suggests that 65 percent will need to achieve immunity through infection or vaccination. In Houston, the figure may be as high as 73 percent because the infection has persisted at a "slow burn" and because of the city’s large, vulnerable Latino and African American populations, who have borne disproportionate risk.
Lee cautions that these results do not mean you can suddenly go to a football game in Houston or Broadway show in New York, but it does mean that with ongoing precautions, the virus might well be contained with the percentages given in her models, until more vaccine arrives.
Though their results vary, most models agree that certain factors are critical, notably age group, which changes the risk of contracting, spreading, and dying from a virus. It's not always predictable: The swine flu, for instance, spared older adults to some degree, while SARS-CoV-2 has severely affected those over 65. Adults 65 and older compose 16 percent of the US population but account for about 80 percent of Covid-19 deaths.
Be Part of the Future
Sign up to receive top stories about groundbreaking technologies and visionary thinkers from SingularityHub.

In addition, age indirectly influences transmission patterns. In 2009, Yale epidemiologists Alison Galvani and Jan Medlock published a mathematical model in Science, showing that targeting flu vaccines to children and young adults (in addition to the elderly) could have slashed swine flu infections from 59 million to 44 million; and for seasonal influenza, 83 million infections could plunge to 44 million. Children, it turns out, drive a disproportionate amount of flu transmission, and protecting them protects society at large.
The study, and others like it, inspired a change in CDC policy to prioritize vaccinating children. "It was a revolution in how we think about vaccines," says Larremore. Vaccination models now routinely consider the power of indirect protection of the most vulnerable by vaccinating those most responsible for spread.
Age also intersects, in complex ways, with social connectivity in different regions. For instance, African American and Latino communities in the United States have been disproportionately hit by Covid-19, in part because of the prevalence of multiple generations living together: Older individuals are much more exposed to the young adults who might be the likeliest carriers of infection.
Modeling connectivity requires drawing grids that represent how we live and move among each other. In 2008, a landmark paper built a grid that epidemiologists everywhere still use today. It stratified people into groups based on age, from birth to 70 years old and up. In the study, more than 7,000 individuals kept a diary of their contacts—nearly 98,000 of them—over the course of one day. Contacts were sorted by place (home, school, work, leisure) and by nature (physical or nonphysical, brief or longer lasting). The model found that 5- to 19-year-olds tend to experience the highest incidence of infection when a new pathogen begins to spread in a completely susceptible population, possibly because of their more frequent and physical contact with others. It also showed how profoundly a society’s grids of connection influence transmission.
The model was expanded globally in 2017, with contact rates for 152 countries. "It’s what we all use," says Matrajt, "because it’s the best thing we have to identify how people contact each other." She incorporated the contact grid into her model.
For example, "if kids are really the hubs around which society is built," Larremore says, "so that if you vaccinate the kids, you fragment that transmission network, then that’s going to give us a totally different way of rolling out this vaccine."
The original grid relied on diaries. Today, our ability to gather data through real time cellphone and online activity may be even greater.
When social distancing became widespread this past spring, it dramatically altered the input into the typical transmission model, says Springborn. Data from the Institute for Health Metrics and Evaluation at the University of Washington shows the power of social distancing in reducing transmission. The contact grids in previous studies are "from pre-pandemic times," Springborn wrote in an email. "We know that contact rates are very different under social distancing and we want to account for that. And we expect social distancing to soften as the number of infections falls. Human nature: As risk falls, so does risk-mitigating behavior."
That needs to be modeled as well. And it will influence the expectations for a vaccine’s rollout and success. In fact, Lee maintains, if we had 90 percent compliance with face masks and social distancing right now, we could contain the virus without a vaccine.
"If kids are really the hubs around which society is built,” Larremore says, “so that if you vaccinate the kids, you fragment that transmission network, then that’s going to give us a totally different way of rolling out this vaccine."
In the study by Springborn, Buckner, and Chowell, social distancing is modeled by creating age-stratified categories for both essential and nonessential workers. Essential workers— health care workers, grocery workers, and many schoolteachers, among others—are at high risk for infection because they cannot socially distance. This model finds that deaths, as well as total years of life lost, are dramatically decreased when essential workers are prioritized to receive the vaccine. Older essential workers between 40 and 59 should be prioritized first if the goal is to minimize deaths, the authors maintain.
With no vaccine, about 179,000 people may die in the first six months of 2021, Springborn says. His team’s model suggests that deaths could decline to about 88,000 simply by introducing a vaccine gradually, giving it to 10 percent of the population each month, and distributing it uniformly without prioritizing any groups. But distributing vaccines in a targeted way, based on people’s ages and whether they are essential workers, could save another 7,000 to 37,000 lives, depending on the situation.
There are other methods of teasing out social connectivity beyond diaries and cellphone data. Census and other data reflect age, profession, and socioeconomic status, and Lee includes them in her models. "The zip code gives you a huge amount of information," she says. Public health data on disease prevalence and hospitalizations can tease out the other unrelated diseases that Covid-19 patients have, as well as vulnerabilities in a given area. Even information on a city’s housing, whether skyscrapers or single-family homes, can give a clue to how closely people are packed together and how likely they are to interact. Inputting this kind of data allows for a vaccine rollout that is sensitive to local conditions. Lee would need to model about 500 representative cities around the US, she says, to cover the country accurately.
....
As powerful as the models can be, they are an imperfect guide. Inevitably they intersect with deep and broad social concerns. The pandemic has disproportionately harmed and killed minorities and those with lower incomes. For that reason, various groups are looking into the ethical principles that should frame vaccine allocation, according to Hanna Nohynek, deputy head of the Infectious Diseases Control and Vaccinations Unit at the Finnish Institute for Health and Welfare, and a member of the WHO’s SAGE Working Group on Covid-19 vaccines.
In the US, the National Academies of Sciences, Engineering, and Medicine has begun to model an equitable allocation of a vaccine. In addition, two other important models have emerged, one associated with University of Pennsylvania School of Medicine, and the other with Johns Hopkins University. Both are guided by concerns about ethics, fairness, maximizing benefits, building trust and the greater public good.
But building trust can be challenging in practice. For instance, it’s widely acknowledged that Black people have experienced hospitalization and death at disproportionately high rates compared to white people. Yet when ethicists begin to talk about prioritizing Black people for vaccines, it can be perceived as an intent to experiment on them by pushing them to the head of the line. If there is concern among African Americans, it’s a logical reaction to "a vast history of centuries of abuse of African Americans in the medical sphere," says medical ethicist Harriet Washington, author of "Medical Apartheid."
Ultimately, both ethical and mathematical models have to face real-world practicalities. "It’s hard because math essentially boils down to a utilitarian calculus," says Lipsitch, the Harvard epidemiologist.
Nonetheless, says Larremore, the models will help guide us in the uncertain early days. "Vaccines take a while to roll out," he says. "We can’t let our foot off the gas the moment a vaccine is announced."
This article was originally published on Undark. Read the original article.
Image credit: Gerd Altmann / Pixabay


Jill Neimark is a writer based in Atlanta, Georgia, whose work has been featured in Discover, Scientific American, Science, Nautilus, Aeon, NPR, Quartz, Psychology Today, and The New York Times. Her latest book is “The Hugging Tree” (Magination Press).
Related Articles

What We Actually See—and Don’t See—Shows Consciousness Is Only the Tip of the Iceberg

These Mini Brains Just Learned to Solve a Classic Engineering Problem

New Device Detects Brain Waves in Mini Brains Mimicking Early Human Development
What We Actually See—and Don’t See—Shows Consciousness Is Only the Tip of the Iceberg
These Mini Brains Just Learned to Solve a Classic Engineering Problem
New Device Detects Brain Waves in Mini Brains Mimicking Early Human Development
What we’re reading